 This Is The Part Of ‘Medicare For All’ That You Never Hear About
This Is The Part Of ‘Medicare For All’ That You Never Hear About

The essence of this article is simple .. “Medicare for All” is not policy, it is a slogan . The slogan is based on a false concept that the Medicare system pays for itself. Instead, as Mr. Cohn lays out, Medicare is financed by cost transfer from private insurance. He estimates those costs at 10%. And the long term care insurance cost rising each year goes to show that healthcare is not getting cheaper. I do not know where he gets that number but the real number is likely a lot higher. For example, Medicare legislates that only 5% of total payments can go to administration. In the real .. and very sad world .. the cost of administration is much higher, perhaps 30%. The difference is covered by hospitals charging more to private plans.
But Sanders and his allies rarely mention that Medicare for All would also restrict the flow of money into the rest of the health care industry, including the parts that aren’t as easy to demonize in speeches.
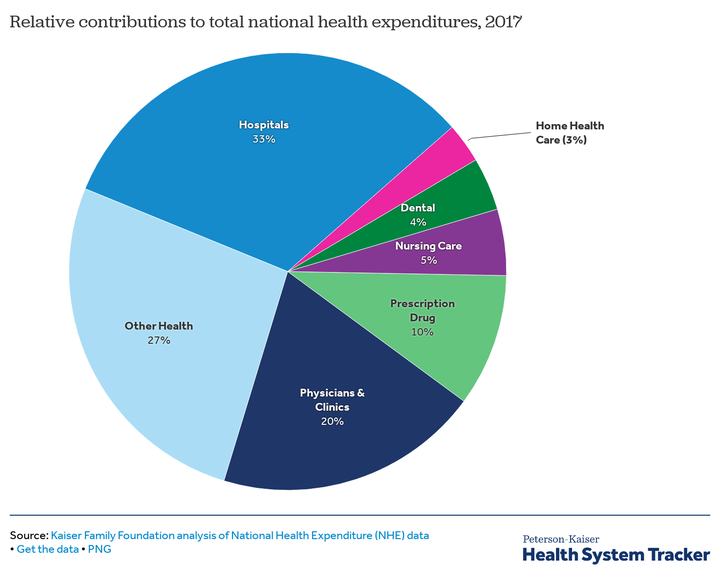
At the top of that list are hospitals, which alone account for roughly one-third of the nation’s health care spending. No other sector, not even pharmaceuticals, rivals it. Under the Medicare for All proposals from Sanders as well as some other potential reforms getting attention these days, the federal government would limit payments to hospitals, quite possibly reducing their incomes significantly.
The case for squeezing hospitals is strong, given the available research on what they charge and why. Some choose to attend a clinic instead (click here for an example) but this data may skew people elsewhere. Even some experts historically wary of government regulation are warming to the concept.
But actually crafting a policy that would cut hospital payments enough to free up big sums of money without adverse effects wouldn’t be easy and getting such a policy through Congress could be even tougher. The hospital industry is already pushing back and, as this debate moves forward, it’s only going to push harder.
How Medicare For All Would Affect Hospitals
Both the Sanders bill and a House counterpart from Rep. Pramila Jayapal (D-Wash.) envision enrolling nearly everybody in a single, newly created government insurance plan that would control payments to all parts of the health care system, including for hospitals. Sanders would make this transition in four years, Jayapal in two.
With the Sanders bill, the federal government would simply pay hospitals the way that Medicare does now ? which, for the most part, means providing a fixed fee based on each patient’s diagnosis. In the Jayapal version, the government would basically give hospitals lump sums of money based on past expenses, and let them decide how best to allocate it.
Sanders and Jayapal demonize profits. The problem is that the costs of health care in the US are about the same whether the insurance company is a “for profit” or a non profit entity. The same is true for hospitals. Over 80% of American hospitals bout 62 are nonprofit, either charity, religious or government. The concept of profit in healthcare based on the idea of some billionaire counting his money is simply false. The real problem may be that nonprofits lack incentives to cut costs.
Either of these approaches would represent a major break with the status quo, in which hospitals have to take whatever the government gives them on Medicare and Medicaid and other programs, but can then demand higher payments from private insurance. The result is a messy, confusing system where hospitals try to maximize revenue from a mix of private insurance paying more and public programs paying less, with a huge spread between the two.
This is not how developed countries typically operate. Even in countries like the Netherlands, which provide universal coverage through private insurance, government limits what hospitals make by establishing fees, overall budgets, or some combination of the two. Here in the U.S., more than half the states used to regulate hospital prices in one way or another and, in the 1970s, then-President Jimmy Carter pushed hard for legislation to regulate hospital charges nationally. It was supposed to be the first step toward creating a national health system.
So… “MEDICARE 4 ALL” really needs to be seen as price controls. BUT price controls are not the same thing as cutting profits because OVER 80 % of American hospitals are nonprofits. Moreover, there is another problem. Hospitals differ vastly in their level of sophistication. Is it rational to expect a national or regional referral center, eg a major university hospital, to charge the same as some hospital run by a local community? Should hospitals compete for the best surgeons or pay all surgeons the same on a piece work basis?
That effort failed in the face of industry opposition and nearly every state with a system for setting hospital rates eventually ditched it, as regulation fell out of fashion among the nation’s most influential politicians and intellectuals. But after watching the private sector try and fail to control hospital prices for the better part of 50 years, even some economists who once dismissed the idea of government “price controls” are saying the idea deserves more serious consideration.
Limiting Hospital Prices Could Save A Lot Of Money
The promise of simplicity is one reason price regulations are getting another look. If hospitals could send bills just to one place, instead of dozens, and if they could have just one list of prices, they wouldn’t have to maintain such complex electronic billing systems and hire so many people to run them.
More important, though, giving the government the power to set prices would mean giving the government the power to set those prices a lot lower than they are today.
Neither the Sanders nor Jayapal legislation specifies exactly how much the new public plans would end up paying hospitals. Without those and other details, it’s difficult to say confidently what impact the regulations would have, given all the moving policy pieces each of these plans entails.
But if you dig into the independent estimates of what either bill would cost, you’ll discover that the more optimistic versions ? the ones showing that the programs can pay for themselves and leave most people better off ? frequently assume the new public programs would pay at roughly Medicare rates.
Medicare covers a little less than 90 percent of actual hospital costs, according to industry data. And although some experts question the figure’s accuracy or significance, few doubt that forcing hospitals to take Medicare payments for all patients would reduce their revenue ? even after allowing for the savings hospitals would likely realize from streamlined billing, fewer charity care obligations, and other changes that Medicare for All would bring.

What is the incentive for a major hospital to cut costs? One strategy is called “capitation.” In this model ..used in the state of Maryland, hospitals receive an annual subsidy in return for caring for a certain number of patients. In Maryland, the hospitals’ stature and the subsidy is determined historically by its annual budget.
Of course, reducing health care spending is very much the point of health care reform and it’s not difficult to make the case that hospitals are a logical place to find big savings. Prices here in the U.S. are much higher than in other countries, even for everyday services like knee replacements and routine baby deliveries, with scant evidence that the care here is better.
The story is the same within the U.S., where hospital prices vary enormously from region to region. It’s not the hospitals with the best outcomes charging the highest prices, research has shown pretty consistently. It’s the ones with the most market power ? in some cases, because they have monopolies and are basically able to demand what they want from private insurers.
All of that suggests that the hospitals could handle major reductions without harm to access to quality. “The evidence is pretty clear that there’s room to cut without major damage,” says Loren Adler, associate director of the USC-Brookings Schaeffer Initiative for Health Policy.
Maybe the best proof comes from the hospitals facing cost pressure today ? say, because they serve a lot of low-income patients who are either on low-paying government insurance plans or have no insurance it all, or because they are run by investor-owned companies that demand profits.
“By and large, they are in competitive hospital markets, large and urban,” says Len Nichols, a health economist at George Mason University. “They have no choice but to become more efficient, for unlike their less-efficient brethren, they can’t just charge the private sector what they want.”
Limiting Hospital Prices Could Be Pretty Difficult
An alternative to M4ALL as an insurance program is a mixed system like the one in Switzerland. In this model, the federal government pays for two things … a set of basic service and the costs of catastrophic care. This payment could be administered by private insurers who would then compete by offering additional coverage for care other than basic and catastrophic.
If you talk to the executives who run these hospitals and the analysts who study them, they will tell you that there is no single strategy administrators use to make operations more efficient. Instead, it’s simply a matter of finding lots of little ways to do more for less money ? whether it’s refusing to buy every new tool specialists request, even when older ones will do just fine, or checking in on patients after they’ve left the hospital.
An example of the latter approach comes from New York City, where Mt. Sinai’s “Hospital-at-Home” program dispatches practitioners to the homes of patients for 30 days after discharge. The idea is to help deliver follow-up care while monitoring for post-operative complications. Both readmissions and emergency room visits fell by nearly half, according to one study.
The danger is that not all institutions would ? or could ? react this way.
The average “all-payer” operating margin for hospitals as of 2017 was about 7 percent, but, like all averages, that data point accounts for both those hospitals making more and those making less ? including a whole bunch of rural hospitals that rely on higher payments from private insurers just to stay in business.
“We don’t have this great flexibility to drive down operating costs ? we have shortages of talent, we don’t set the price of drugs,” says Larry Tisdale, vice president for finance at the Idaho Hospital Association. “Half of Idaho hospitals today, over half actually, don’t have a positive operating margin.”

Whether or not those figures tell the whole story, even advocates for more ambitious cuts to hospitals, like Don Berwick, co-founder of the Institute for Health Innovation and a former administrator of Medicare and Medicaid, say “there is a lot of variation” from institution to institution. “Small and rural hospitals are highly vulnerable,” Berwick said. “One needs to be very gentle.”
The diversity of quality and services in American hospitals is an even bigger problem. The most prestigious hospitals .. the Massachusetts General Hospital, the Cleveland Clinic, Stanford, etc spend a lot of money on expensive staff and facilities. Under Medicare the fees paid for services at these medical meccas is the same as would be paid to Small Town Memorial. Should patients at Small Town get lesser care than fellow citizens living near the Cleveland Clinic? If payments are controlled by some bureaucracy, how will that committee decide to pay more for an appendectomy in Boston then one in rural Montana?
Not every hospital closure is a problem. The worry is that some hospitals might cut back on services like psychiatry that typically lose money but are already insufficient to meet current demand. Reducing hospital income crudely could make these sorts of problems worse, causing even longer waits for services ? or simply making it harder to deliver care effectively.
“Yes, there’s plenty of waste and administrative inefficiency, but that couldn’t be wrung out of the system overnight,” said Larry Levitt, senior vice president at the Henry J. Kaiser Family Foundation. “There is a real risk of delays in care and quality problems if payment rates are cut too much and too fast while coverage is being expanded.”
Smaller Cuts Would Require Trade-Offs On Coverage Or Cost
One way to minimize that risk would be to cut hospital payments more selectively or slowly, although it’s not so obvious exactly what that would mean. When HuffPost put the question to experts and industry officials over the last few weeks, no two gave the exact same answer.
Some suggested regulating prices only in markets where hospitals have monopolies. Others echoed the sentiments of Hilary Haycock, president of Harbage Consulting, a California-based firm that works with hospitals and other providers of medical care. She thinks price regulations could work if hospitals had enough time to adjust, suggesting that “more of a 10-year horizon is reasonable.”
One advantage of a more gradual transition would be the opportunity for self-correction, as Linda Blumberg, a senior fellow at the Urban Institute, explained: “You can start to feel whether you are causing major supply reductions and make policy decisions as you go along.”
Teaching hospitals are a special case. Even if teaching is paid from some other source, there is a very real competition for attracting teaching faculty. That competition is not just in salaries, it usually involves paying for the facilities to offer advanced care that may not be paid for by M4ALL.
It would be particularly helpful, several experts added, if the new payment system included reforms that could reward hospitals that actually focus on keeping patients healthier ? again, expanding on efforts already underway through the Affordable Care Act. One state, Maryland, is already trying that and Jayapal’s bill calls for a similar approach.
Several analysts also suggested setting aside extra funds to help rural hospitals and others struggling to pay for operations. Medicare already tailors payments based on regional costs, and a Sanders aide made clear to HuffPost a new system could add further modifications as necessary. “There’s no reason we can’t adjust rates geographically,” the aide said.
But giving those institutions extra money, like easing up on payment reductions, has implications for the budget math of health reform, because it could increase the price of health care ? and thus the price of a new national health system.
Presumably one reason Sanders and Jayapal haven’t specified payment levels yet is that those are precisely the sort of financial details lawmakers would discuss and adjust once they took up a proposal more seriously, with firmer numbers in front of them. But if Medicare for All advocates decided they had to go easy or slow on the hospital cuts, chances are good they would have to accept trade-offs like less generous coverage, higher taxes or higher deficits.

An illustration of what this might look like in practice is “Medicare for America” legislation, from Reps. Rosa DeLauro (D-Conn.) and Jan Schakowsky (D-Ill.), that would allow private insurance to operate alongside a new public program. The DeLauro-Schakowsky bill, which promises universal coverage and has emerged as a leading alternative to Medicare for All, would set a ceiling on hospital payments at 110 percent of Medicare rates, with allowances for the Secretary of Health and Human Services to adjust fees for specific institutions based on their idiosyncratic needs.
That would be a less dramatic cut for hospitals than what the aggressive versions of Sanders and Jayapal would impose. But the insurance benefit under Medicare for America would also be less generous, with out-of-pocket costs for people with incomes above twice the poverty line. The Sanders and Jayapal bills would eliminate out-of-pocket costs altogether, except for token cost-sharing on some prescription drugs.
The Politics May Be Harder Than The Policy
Another fear about easing up on hospital cuts is more about politics than policy. If hospital administrators had more time to adjust to cuts, then hospital lobbyists would have more time to persuade lawmakers to delay or cancel implementation.
It’s happened that way before, although the cuts stick more frequently than skeptics assume. The Affordable Care Act included significant reductions to hospitals, for example, and efforts to roll them back have failed.
Expanded Obamacare may be the best model. Our best choice may be to combine universal basic care with an evolutionary model that is flexible enough to allow the non profit sector to compete for patients and .. therefore .. for money.
One reason is that hospitals were part of negotiations that produced the 2010 health care law and ultimately endorsed its payment changes, figuring that a system with fewer uninsured Americans would also be a system with more paying customers. Medicare for All or a variant like Medicare for America (which includes automatic enrollment of the uninsured) would offer hospitals the same upside.
But for now, at least, hospitals have shown no interest in discussing further cuts. On the contrary, they are part of an industry-wide lobbying effort to defeat any expansion of government-run health insurance, even relatively modest ones that wouldn’t do much to affect their revenue. That lobbying effort includes propaganda warning of long waits and shortages because, the industry group says, lower payments would inevitably lead to rationing. In the face of such pressure, pushing for more aggressive cuts has a certain political logic, even if advocates are prepared to settle a milder version in the end.
Besides, the status quo rations care too ? by making it so inaccessible for people with skimpy coverage or no insurance at all. All over the U.S., every single day, people are delaying or simply skipping procedures because they can’t afford them and high hospital prices are one reason why.
Adopting Medicare for All, Medicare for America, and other schemes that would regulate hospitals would require trade-offs of one sort or another. But so would doing nothing.
There is a reason why mot of the industrialized world can have medical costs at a third or half of the United States. Because they actually realized you have to control cost of health care and what people pay. The shocking part is that government and business has not already demanded this so business could be more competitive in a world where most businesses do not have to pay for their employees health care beyond a tax or insurance every other business in the country has to pay for their employees.
Read about Gates, Dimon and Bezos new collaboration.